
What Happens when You are The Doctor on the Airplane?
My friend Drew is a doctor. I am not.
Recently he posted a note to Facebook that he had been summoned into action onboard a flight. He was the doctor who responded when they asked over the speaker, "Is there a doctor in the house?" I couldn't let that story go untold, so I sent him a bunch of questions, which he was kind enough to answer.
Rob Cockerham: You are a doctor, how long have you been a doc and what is your specialty?
Dr. C: I "officially" became a doctor (i.e., graduated from medical school) in 1995. I am an anesthesiologist and have been since 2004. Prior to that I trained for several years as a general surgeon before switching specialties.
Rob: Where were you headed? Was it business or pleasure? Were you alone on the flight?
Dr. C.: The flight was on Thursday, October 18. American Airlines flight 245, from DCA (Reagan National Airport in Washington DC) to LAX, an early evening flight. I was returning home from attending the American Society of Anesthesiologists annual meeting, so I guess this qualifies more as business than pleasure. I was flying by myself in seat 6B, the last row in first class.
Rob: How long into the flight did the emergency develop, and how did you become aware of it?
Dr. C.: We were approximately 2.5 hours into the 4.5 hour flight when a flight attendant asked if there were any physicians on board the plane that would identify themselves by pressing the flight attendant call button. I distinctly remember her not mentioning any kind of medical emergency, but she said something about having a "medical question". She was very calm about it.
Rob: What was the nature of the emergency? Was it life-threatening?
Dr. C.: After I pressed the flight attendant call button, she asked me to come to the fore galley (right behind the cockpit) where she notifed me that one of the passengers, also in first class, was having a bit of respiratory distress, likely from an allergic reaction. The woman was seated just 2 rows in front of me, in 4E. I would describe her as tall and heavy-set, and probably weighed around 275-300 pounds.
One thing I noticed during boarding was that after sitting down, this woman had immediately called the flight attendant over and told her that she had an extreme allergy to shellfish and fish, and that the menu for the flight in first class featured shrimp as an appetizer. She was pretty persistent to the point of being pushy - insisting that the flight attendants wash their hands every time before even walking by her seat! I could tell the flight attendant was annoyed at this request but she didn't make a big deal out of it.
Rob: Were you the only doctor on the flight?
Dr. C.: At the time, I was the only one who identified as a physician. However, after we landed another passenger came up to me and told me he was a doctor too (in fact, he was also an anesthesiologist returning from the same convention), but he had slept through the entire incident!
Rob: Did you treat her at her seat, or lying down in the aisle?
Dr. C.: She was treated while sitting in her seat the entire time. If she needed to, she could have laid down in the aisle but nobody would have been able to get by.
Rob: What did you do?
Dr. C.: The first thing I did was introduce myself, ask what the problem was, and then tried to find out as much as I could about her medical history. She told me about her allergies, and that the last time she had a severe allergic reaction, she had gone into cardiac arrest and required CPR (definite cause for concern because that gives me a good indication of how severe her reactions are to an allergen). Her primary complaint was that she was having difficulty breathing because she felt her airway swelling up. She blamed the shrimp - even though she didn't eat or touch any, it was quite possible that she was exposed to small particulates in the air. Being in a pressurized fuselage with recirculated air probably didn't help matters any.
I suggested was that she take some oral Benadryl (an antihistamine) and try to relax a little bit, which she agreed to. I got a few Benadryl capsules from the medikit and gave it to her, and I told her that I'd check back with her in 15-20 minutes to see if she felt better. Since I was sitting just 2 rows behind her I didn't think I needed to stay next to her the entire time.
After about 15 minutes, she was still having difficulty breathing, so at that point I suggested giving her some oxygen, starting an IV, giving some fluids, and administering a little IV Benadryl to see if it would work faster than oral medications. About 5 minutes after I did this, she complained about feeling worse so I administered a shot of epinephrine (luckily, she had carried 2 Epi-Pen vials on board with her) in her thigh, which freaked her out but she felt a little better after that.
About 30 minutes before landing at LAX, she began complaining of chest pain and heart palpitations (which can happen with epinephrine), but since we were on approach by that time I just tried to calm her down.
Rob: What was the first aid kit like? Obviously they can't bring everything, but are there any improvements you would make?
Dr. C.: I was surprised! The medikit was actually really comprehensive - it's about the size of a small backpack and has compartments that contained oral medications like Tylenol, Benadryl, Aspirin, etc. as well as IV lines and fluids, a tourniquet, a stethoscope, AED, blood pressure monitor, syringes and needles, and a decent stock of emergency IV drugs like dextrose (for low blood sugar), epinephrine, atropine, and even morphine. There was also a small portable cylinder of oxygen and a mask that the patient used for the remainder of the flight.
The only device I wished the medikit had was a pulse oximeter, which is a small probe with a red LED that clips on a finger. It measures oxygen saturation, which in this case would be a good indicator of a patient's ability to breathe and exchange gas effectively in the lungs.
Another thing - before I was allowed to open the medikit, I had to get an OK from the physician on the ground that the flight attendants were communicating with. US airlines are contracted with a service called Medlink that has a physician on the ground, on call 24 hours a day, just to handle issues like this. This physician has the discretion to recommend that a flight divert to a nearby airport if necessary, as well as defer medical treatment decisions to other doctors on board the flight (as in this case).
Rob: Did you make any requests from the passengers, like "I need a tiny rubber band! Someone! Hurry!", or motion for all the other passengers to be perfectly quiet? Was anyone A) freaking out or helping you?
Dr. C.: The rest of the passengers on the flight were great. Nobody freaked out and most just went about their business, but looked ready to offer assistance if I had asked for it. As for me, for about an hour and a half I was constantly moving from my seat to the woman's seat to check on her, to the fore galley to get stuff from the medikit, talk to the flight attendants, etc.
Rob: Was it peanuts? I bet it was peanuts.
Dr. C.: Good guess, but no - it was shrimp/shellfish.
Rob: Honestly, isn't this exactly the reason you became a doctor?
Dr. C.: Heh, not really, but I was very happy to help out. One thing I realized from this experience is how helpless one can feel being 35000+ feet in the air when something goes wrong.
Rob: Did the other passengers break out in applause when it was over?
Dr. C.: No, no applause. However, when I was leaving the plane with the patient and the paramedics (the flight attendants had asked everyone to wait until we got off first), a lot of people I passed by did have complimentary things to say, which was nice.
Rob: Did the flightplan change to treat her emergency?
Dr. C.: No, but during the incident the captain did ask me if I felt we should divert to Denver or Phoenix. I decided it wasn't necessary because the woman's vital signs were stable, and I felt I could manage her issues until we landed at LAX. Additionally, diverting the flight meant inconveniencing the 100+ other passengers on the plane as well as costing AA thousands of dollars, but if I felt we had to divert, I wouldn't have hesitated to tell the captain to do so.
Rob: Did you end up getting sued?
Dr. C.: No, I didn't. In fact, this article mentions that no physician has been successfully sued for assisting in an inflight medical emergency: http://methodistanesthesia.com/Articles/Article_25.pdf
Rob: Did the staff of the aircraft, airline, patient, other passengers, etc., thank you?
Dr. C.: Yes, as you probably saw from my FB feed, I received a nice email from the director of medical and occupational heath services at AA as well as 25000 AAdvantage frequent flyer miles. If you'd like a copy of the email just let me know.
Rob: Respecting her privacy, was there a patient aftermath?
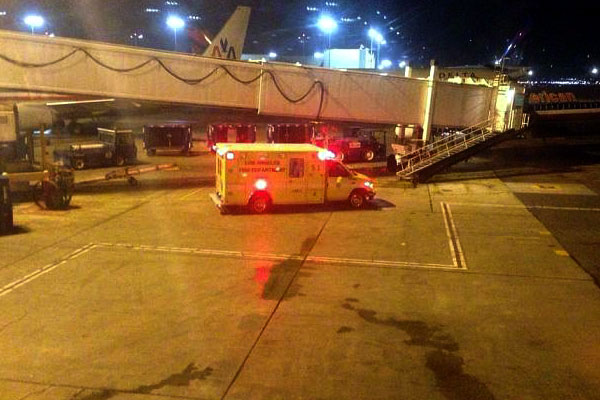
Dr. C.: Unfortunately, I don't know what the outcome was. As we got off the plane I told the paramedics exactly what happened and what was done, and they took it from there. The patient was placed in a wheelchair and taken to a local hospital (I presume Centinela Hospital, which is the closest hospital to LAX).
Rob: Did you miss half of your inflight movie?
Dr. C.: I missed the entire movie! That's OK though, on planes I'm usually plugged into my own iPod or iPad for inflight entertainment.
Rob: Would you do it again?
Dr. C.: Absolutely. Sometimes it's hard to appreciate all the schooling and training you've undergone until you're faced with a situation like this. Ultimately, the feeling you've helped someone out and made a difference in their life is the best reward.